Welcome to Anderson Podiatry Center!
We’re excited to meet you and partner with you on your journey back to full health—whether that means returning to work, enjoying life, or getting back to the activities you love.
Your Visit to APC
Our friendly and knowledgeable office team is here to answer any questions you have about foot and ankle conditions, as well as chronic pain affecting your body. To ensure your first visit goes smoothly, please review the information below.
Convenient Locations
Anderson Podiatry Center serves you from four easily accessible locations, including Fort Collins and Broomfield, Colorado. Click here for maps and directions.
New Patient Forms
Please arrive 15 minutes early for your first appointment to complete necessary paperwork.
Additional forms, such as the Medical Records Release Form, should only be completed if directed by our staff. You can download and print these forms ahead of time to bring with you.
Insurance and Payments
We accept most insurance plans—including Medicare, Anthem Blue Cross and Blue Shield, and many government programs—and will verify your benefits before your appointment.
We also accept checks and major credit cards, with financing options available through CareCredit to help make your care affordable.
We look forward to helping you thrive with expert foot care and personalized support every step of the way.
A year ago, Ella was just five days out of surgery after undergoing a nerve decompression procedure, and the change in her life was already remarkable. Before the operation, she had been suffering from severe sleep deprivation, only managing around five hours of sleep a week. This level of exhaustion had become her norm, and the toll it took on her physical and mental well-being was immense. However, within just five days post-op, Ella was already experiencing significant improvements. She was finally able to sleep through the night, something she hadn’t done in years.
Now, one year later, Ella’s progress continues to astound. The nerve decompression procedure has had a lasting impact on her quality of life, restoring a sense of normalcy she hadn’t thought possible. Before, the constant pain and discomfort had severely limited her ability to rest, leading to overwhelming fatigue. However, since the surgery, Ella’s sleep has dramatically improved, and she’s been able to enjoy peaceful nights of uninterrupted rest. Not only has her sleep returned to a healthy pattern, but the nerve-related pain that once dominated her life has subsided, giving her the freedom to focus on other aspects of her health and happiness.
This follow-up story with Ella offers insight into the long-term benefits of the nerve decompression procedure. Her recovery journey highlights the procedure’s effectiveness in reducing nerve pain and improving sleep. For those considering similar treatments, Ella’s experience serves as a powerful example of the lasting relief and improved quality of life that can come from addressing nerve compression issues through surgery.
Heel pain is one of the most common complaints that foot specialists encounter. Many people assume that pain in the bottom of the heel is caused by plantar fasciitis, which is true for most patients. However, another less common issue, known as heel pad syndrome, can also cause heel pain. In this blog, we will discuss the causes and treatment of heel fat pad syndrome. Additionally, you may have received a misdiagnosis, and we will explore a little-known condition that could explain why your treatments have not been successful.
The Basics: Heel Anatomy
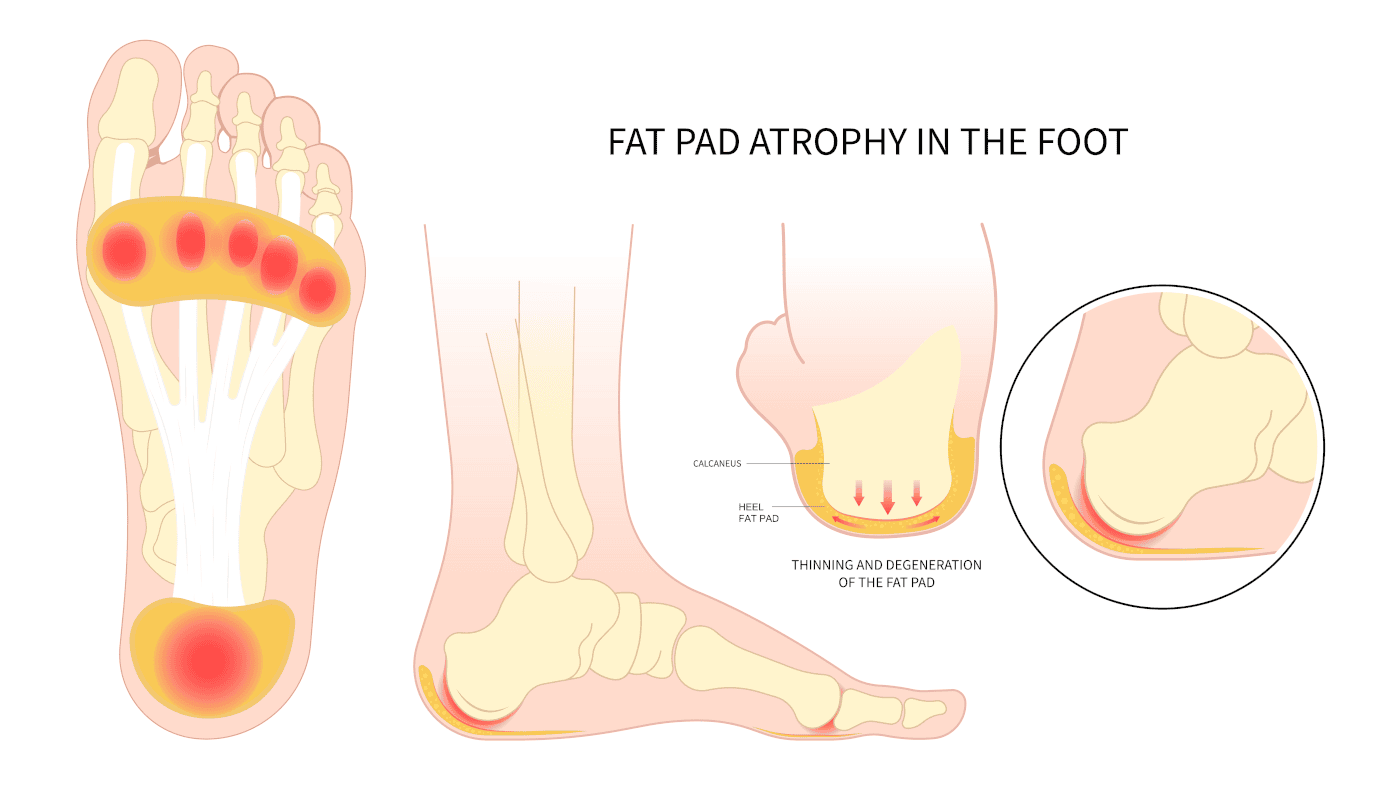
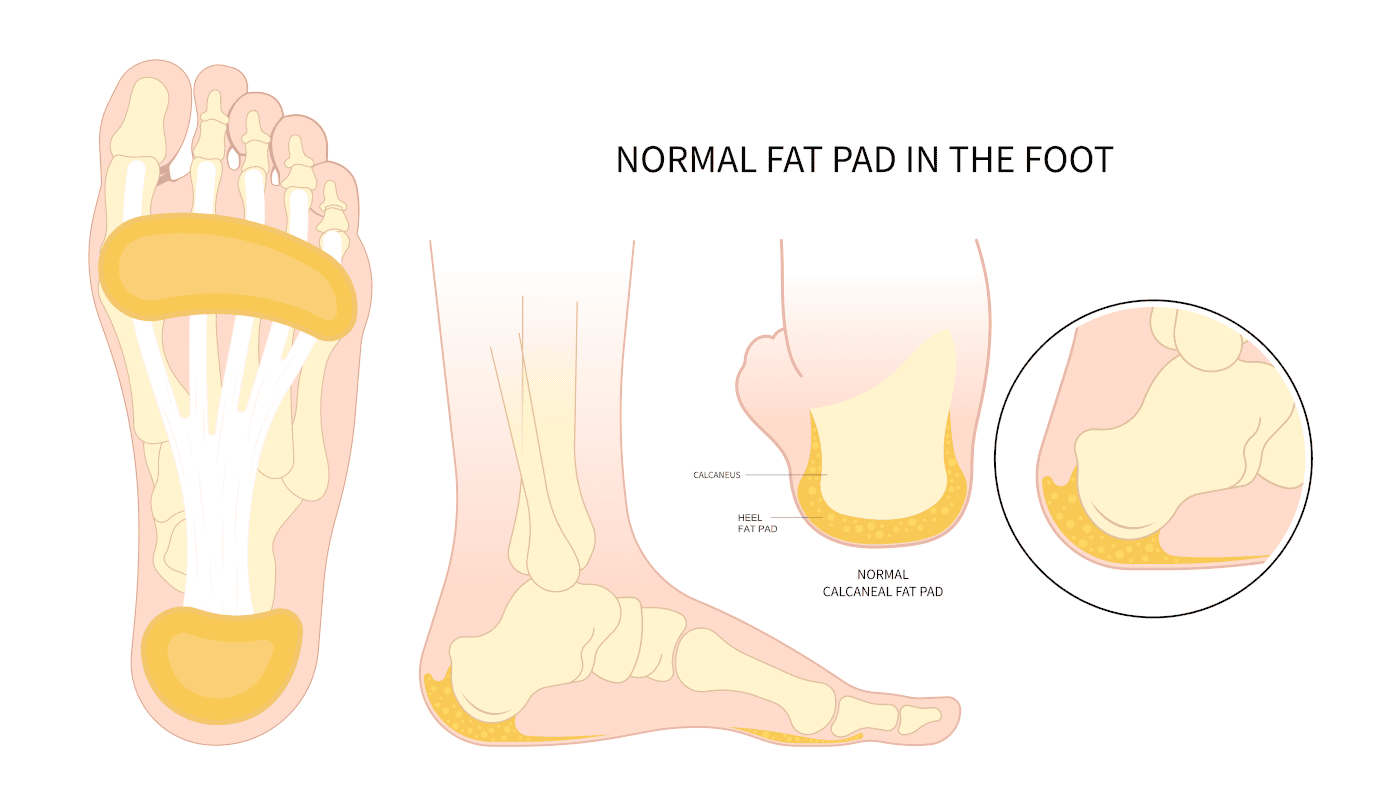
The foot is uniquely designed to absorb shock. As we walk or run, the foot strikes the ground with 3-4 times our body weight. To compensate for this, the heel, the softest bone in our body, dissipates that shock. Beneath the skin, a significant amount of fatty tissue is distributed throughout the bottom of the foot, providing additional cushioning.
Within the fat are tight connective tissues that act as a net to support the fat pad’s structure. On the bottom of the heel, x-rays may reveal a heel spur. Using ultrasound technology, a podiatrist can also detect abnormalities in the plantar fascia.
The plantar fascia originates in the ball of the foot, extends through the arch, and inserts at the bottom of the heel. With every step, the arch flattens, causing the fascia (a tight connective tissue) to pull on the heel.
Symptoms of Heel Pad Syndrome
When one is suffering from heel pad syndrome, the pain will be directly underneath the heel bone. Pain may be present first thing when you get up in the morning or when you walk throughout the day. The pain will not extend to the arch but is centered directly underneath the heel.
Causes of Heel Pad Syndrome
Heredity – Some people may inherit a thinner fat pad from their parents.
Cortisone Injections – Cortisone injections, which doctors may use to treat plantar fasciitis, can lead to heel pad syndrome and contribute to fat pad atrophy.
Hard Surfaces – Walking or running barefoot, as well as engaging in activities on hard surfaces like concrete or wooden floors, can cause the fat pad to thin.
Biomechanics – Certain foot structures are more likely to cause fat pad atrophy.
Excess Body Weight – People who carry more body weight may increase their risk of developing heel pain. The added weight stresses and displaces the fat pad.
Age – As we age, the fat pad naturally thins as part of the aging process.
Metabolic Problems – Medical conditions like type 2 diabetes, lupus, and rheumatoid arthritis can increase the risk of developing heel pain.
Diagnosis of Heel Pad Syndrome:
Symptoms – The doctor asks you about your symptoms, where they are located, and when they occur.
Examination – The doctor examines your foot to determine where the pain is located.
Testing – The doctor may take X-rays to rule out any bony involvement.
Diagnostic Ultrasound – The doctor uses ultrasound to measure the thickness of the fat pad and evaluate the plantar fascial tissue in the affected area.
MRI Imaging – The doctor may order an MRI to assess the fascia and fat pad, and more importantly, to rule out a stress fracture in the heel.
Treatments may include the following:
Shoe Gear – Wearing shoes with extra cushioning can help provide relief.
Heel Cups – It will help center the fat directly beneath the heel, preventing displacement from the middle when you bear weight.
Medication – Taking anti-inflammatory medications can help reduce pain and inflammation.
Icing – Applying ice can alleviate symptoms in mild cases of heel pad syndrome.
Shoe Inserts – Using over-the-counter arch supports or custom-made orthotics can offer additional support and comfort.
Life style Changes:
Avoid High-Impact Activities – Avoid high-impact activities like basketball that cause heel pain. Jumping and landing on your feet wear down the fat pad. Instead, opt for low-impact activities that involve softer surfaces like swimming.
Maintain a Healthy Weight – Keeping a healthy weight reduces the impact and force on your feet, allowing for better distribution and control.
Why the diagnosis of Heel Pad Syndrome should throw up a red flag in your mind?
Plantar Fasciitis – When it comes to pain in the bottom of the heel, the most common diagnosis is plantar fasciitis. To accurately diagnose this foot problem, patients with heel pain should undergo a diagnostic ultrasound. Using an ultrasound, a podiatrist can evaluate both the appearance and thickness of the fascia to confirm the diagnosis. Without this test, a definitive diagnosis cannot be made.
Heel Spur – Heel spur pain is a common misconception. In the past, people believed that if a heel spur appeared on an x-ray, it was the source of pain. However, with the introduction of endoscopic surgery in the late 90s, this belief has become outdated. This advanced technique, which has proven highly successful in eliminating heel pain, changed the understanding of heel spur pain.
During this procedure, surgeons make small incisions on both sides of the heel, allowing them to visualize and cut a portion of the fascia to relieve tension. Interestingly, the success of this technique does not involve removing heel spurs, even though many patients undergoing the procedure have heel spurs. As a result, the idea that heel spurs cause pain has been invalidated. In fact, as early as the 1930s, medical literature stated that heel spurs develop due to the fascia pulling away from the heel, but the spur itself does not cause pain.
Your Fat Pad Syndrome Pain may truly be Nerve Pain. Are you misdiagnosed? Your Fat Pad Syndrome may be Nerve Pain.
The Medial Calcaneal Nerve Branch
The medial calcaneal nerve branch passes beneath the heel bone, located precisely where the pain occurs. This nerve originates from the posterior tibial nerve, which travels along the inside of your ankle. The posterior tibial nerve has branches that supply sensation to the bottom of the foot, much like the carpal tunnel area in the hand. Specifically, two branches in the tarsal tunnel extend to the arch and ball of the foot, providing sensation to these areas.
Meanwhile, the third branch, the medial calcaneal nerve, travels down the inside of your heel and supplies sensation to the bottom of the heel bone. On its way to the heel, it passes through a small tunnel on the inner side of the heel bone. This tunnel, composed of tightly connected tissue, can entrap or compress the nerve. Additionally, when the plantar fascia thickens in patients with plantar fasciitis, this nerve often becomes irritated. As a result, a patient may experience both plantar fasciitis and nerve pain simultaneously.
Diagnosis of Medial Calcaneal Nerve Branch Pain
Clinically – The doctor evaluates the heel by checking for discomfort, which usually occurs on the inner side of the heel bone.
Diagnostic Injections – The doctor may administer an injection at the entrapment site of the nerve. The location is on the inside of the heel and then it follows beneath the heel bone. When patients respond favorably with a significant reduction in pain, this confirms the diagnosis.
Treatment
Cortisone Injections – Doctors can use cortisone injections to help confirm the diagnosis, and a series of two or three injections can eliminate the pain.
Radio Frequency Nerve Ablation Technique – This technique effectively blocks the pain signals in the nerve.
Surgery – As a last resort, surgeons can resect the nerve and bury it into the muscle in the lower leg.
Have you been told you have heel pad syndrome and the attempts by your doctor have failed? Please consider the little-known diagnosis of medical calcaneal nerve branch entrapment. This may truly be what is slowing you down and causing your heel pain. This is why you should contact our certified foot doctors.
Pain in the arch of the foot is a very common complaint seen by podiatrists. One of the most common causes is plantar fasciitis. This blog will discuss many other potential causes of arch pain that you may not have heard of. If you are having arch pain and are frustrated with what you have tried or what your doctor has tried and this problem persists, this blog is for you. We will go into more detail as to other causes that may lead to arch pain. It is important to get to the root cause for your arch pain to resolve.
The Basics of Arch Pain in Foot
Let’s first explain what the arch on the bottom of the foot is composed of.
Plantar Fascia. Beneath the skin is a strong connective tissue that goes from the ball of your foot to your heel, and it is called your plantar fascia. As we get older, the fascia becomes less elastic but as a young person, it has more elasticity and if we step down on the foot the fascia has the ability to elongate. This flexibility is lost over time resulting in the pulling of the fascia from where it attaches to the heel bone.
Nerves. Deeper to the fascia are multiple nerve branches that supply muscles in the arch and also the skin. The nerves originate from your back and on the pathway to get to the bottom of your feet, the nerves pass through two nerve tunnels. One nerve tunnel is called the soleal sling in the upper calf and another nerve tunnel in the inside of the foot, in the ankle region is called the tarsal tunnel.
Musculoskeletal. The musculoskeletal aspect of your foot refers to the muscles, the tendons, the bones, and joints. These could also be the cause of arch pain.
Why am I getting arch pain?
There are multiple things that you could have done that lead to pain in the arch. These include the following:
Shoes that have been overused and are breaking down. Wearing shoes that do not provide adequate support can cause multiple problems in your feet. This may occur because the shoes do not provide adequate support or have broken down.
Overtraining. Maybe you are starting to do more rigorous activities such as running, walking for more days a week, or hiking. It is important to have rest days between the days you are stressing your body or do alternative activities on those days so that you are not overstressing your feet. When you start to feel pain, using ice packs to apply ice and taking anti-inflammatories may be helpful to relieve pain and reduce swelling if you are overtraining. Icing can be done for up to 20 minutes at a time.
Foot type. Some feet structurally are more susceptible to arch pain, and this can include flat feet but also a very high arch foot. Both may lead to arch pain.
Specific Causes and Treatments for Arch Pain in Foot
Plantar Fasciitis
Plantar fasciitis may be the most common cause of arch pain, and it is the most common terminology used by the public and healthcare professionals. However, because of this, the diagnosis may be overused and especially if you are not seeing a foot specialist and not getting better, you should start to question the diagnosis, and you may want to consider getting a second opinion.
Where is Plantar Fasciitis located?
With very few exceptions, plantar fasciitis is closely located where it is inserted in the heel. People present with pain in the bottom of the heel when they first get up in the morning and bear weight. As the arch flattens, the plantar fascia is pulled, and it is believed that microscopic tears can be created at the juncture where the fascia attaches to the heel bone. It may also occur in the middle of the foot, but it is much less. This is important to note because if the pain is in the middle of the foot, other problems may be the cause.
Treatment for Plantar Fasciitis
Treatment can involve more supportive shoes, or a podiatrist may recommend custom-made supports called orthotics. Other treatments such as regenerative medicine where human cellular tissue products are used to repair the damaged fascia at its connection of the heel bone can be utilized. Some patients have also found that icing, resting, and using over-the-counter inserts may be helpful. Finally, physical therapy using stretching and strengthening exercises may also be useful. After all conservative measures have failed, endoscopic heel surgery may be performed to release a portion of the fascia so that it can elongate and therefore reduce its pulling from the heel.
Nerve Conditions
Tarsal Tunnel Syndrome
The tarsal tunnel is an area where all the nerves on the bottom of the foot need to pass through to supply the bottom of the foot. It is located on the inner side of the foot below the ankle bone. Much like carpal tunnel syndrome in the hand, if this tunnel is tight, you may get symptoms of burning, tingling, and numbness in a portion of the arch, or in the entire bottom of the foot. Treatments for tarsal tunnel syndrome may include custom-made arch supports, cortisone injections may be used to help diagnose but seldom reverse the symptoms, laser treatments may also be effective. If symptoms are unresolved and severe, surgical decompressing (opening) of the nerve tunnels in that area may be needed to be performed much like doing carpal tunnel in the hands.
Soleal Sling Entrapment
Another nerve condition can create symptoms in the arch from a nerve tunnel located in the upper calf area. The main nerve that supplies the bottom of the foot is called the tibial nerve and it is a branch of the sciatic nerve. It passes through a tunnel that is located where the soleus muscle originates in the upper calf. The soleus muscle which inserts in the Achilles tendon originates in this area and where its origination is a fibrous band that can entrap (compress) the nerve. This band is referred to as the soleal sling. The symptoms from this can create burning, tingling, and numbness of the foot and the arch, and it occurs more with activity and dissipates with less activity. It is also found to cause significant cramping in the arch. Very few health professionals are adequately trained to evaluate and treat this problem, and many are unaware of its existence as a possible cause of arch pain. Treatments for soleal sling entrapment would include laser treatment, electrical stimulation treatments, cortisone injections which may help temporarily, and if symptoms are severe and chronic, surgical decompression (opening) of the tunnels may be needed.
Musculoskeletal
Stress Fractures – For some, a stress fracture in the bones of the arch of the foot or the long bones in the foot called the metatarsals can lead to arch pain. Although rare, there are situations where a stress fracture in the arch of the foot can cause cramping of the muscles thus causing pain in the arch. The cramping is present because the body is trying to splint or immobilize the bone because of the fracture. This is nature’s way of attempting to reduce stress on the bone and thus help the bone to heal.
Tendons – There are areas in the arch where important tendons attach to the foot. If these tendons become overused there can be mild tears where they connect to the bone. For treatment, it is important to properly diagnose with an ultrasound evaluation or an MRI. In many cases, custom-made arch supports can eliminate the pain and in other situations, regenerative medicine can be used to repair the damage to the tendon or surgery may be necessary.
Arthritis – There are multiple joints in the mid arch of your foot that are formed by the tarsal bones and the articulation of the tarsal bones with the metatarsals. As we get older, these joints may become arthritic and the body’s response to arthritis is splinting of the muscles in the arch to immobilize the joints, and this can help reduce the pain. Pain may also be noted on the top of the foot but also on the bottom of the foot in the arch. Treatment for this is more supportive shoes, custom-made arch supports, surgery to fuse the joints, and also regenerative medicine can help reduce joint pain.
Severe Flat Feet
Finally, it must be mentioned that there are situations where a foot may be severely flat and most conservative measures may fail and because of this, a podiatrist may need to consider the option of surgery. With a severe flat foot, there could be severe stress or strains on tendons, nerves, and joints where surgical correction would be the preferred treatment plan.
If you are having arch pain that is getting unresolved, make sure to consider many of the other possibilities besides plantar fasciitis. Plantar fasciitis is a big buzzword in healthcare, and it is important that you are armed with this information so that you can get the best treatment possible for your arch pain if you are not responding to the present treatment plan you are going through. And finally, you may want to consider consulting with a board-certified peripheral nerve surgeon as seeing this type of specialist would be best if you are suspicious of nerve involvement as mentioned in this blog. In summary, please consider visiting The Association of Extremity Nerve Surgeons to find peripheral nerve surgeons in your area.
Book your appointment online or call our Fort Collins and Broomfield, Colorado foot and ankle specialists at the clinic nearest you.
Frequently Asked Questions About Foot Arch Pain
What are the most common causes of foot arch pain?
Common causes include plantar fasciitis, nerve conditions like tarsal tunnel syndrome, poor footwear, overtraining, and certain foot types like flat feet or high arches.
How do I know if my foot arch pain is due to plantar fasciitis or something else?
Plantar fasciitis usually causes heel pain when first standing in the morning, while persistent arch pain, burning, or numbness may suggest a nerve issue like tarsal tunnel syndrome.
Can wearing the wrong shoes lead to foot arch pain?
Yes — worn-out or unsupportive shoes can cause or worsen arch pain by failing to provide the necessary support for your foot’s natural structure.
When should I consider seeing a specialist for foot arch pain?
If your arch pain persists despite rest, better footwear, and home treatments, or if you’re unsure of the diagnosis, it’s wise to see a podiatrist for a thorough evaluation.
What treatment options are available for chronic foot arch pain?
Treatments range from orthotics, physical therapy, and regenerative medicine to nerve decompression surgery, depending on the underlying cause.
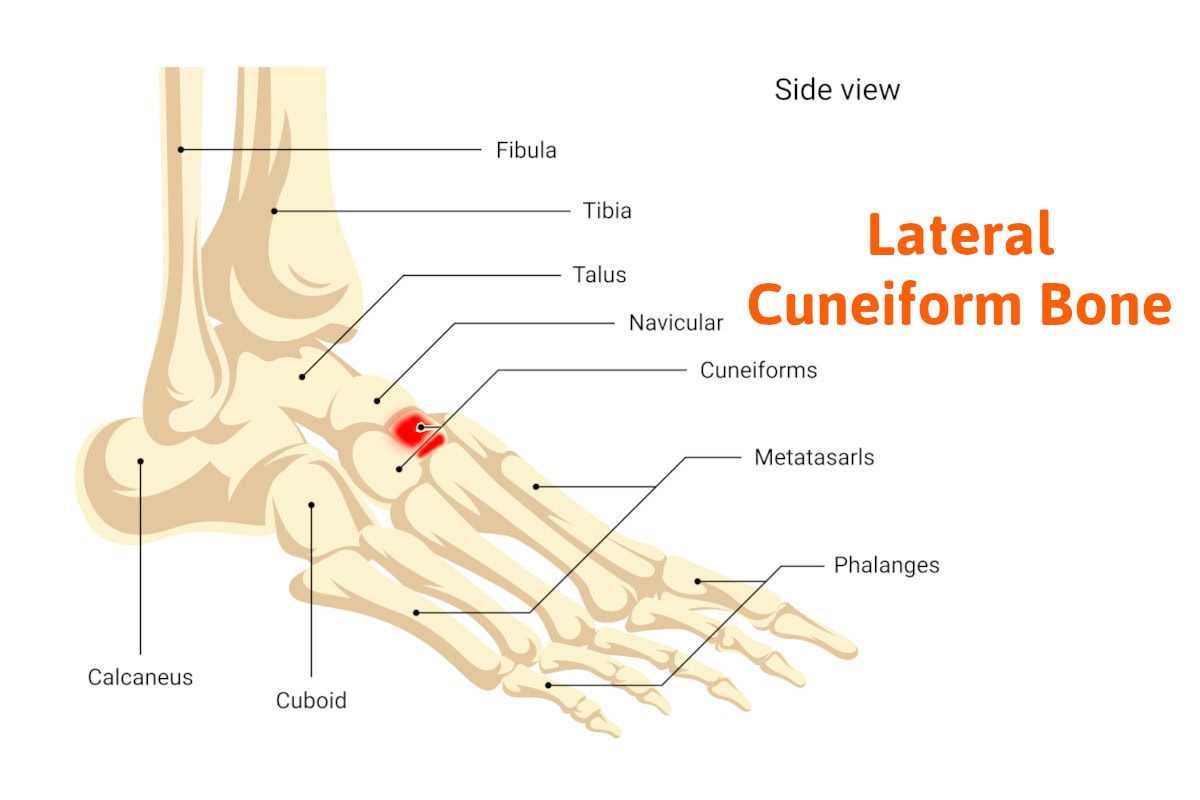
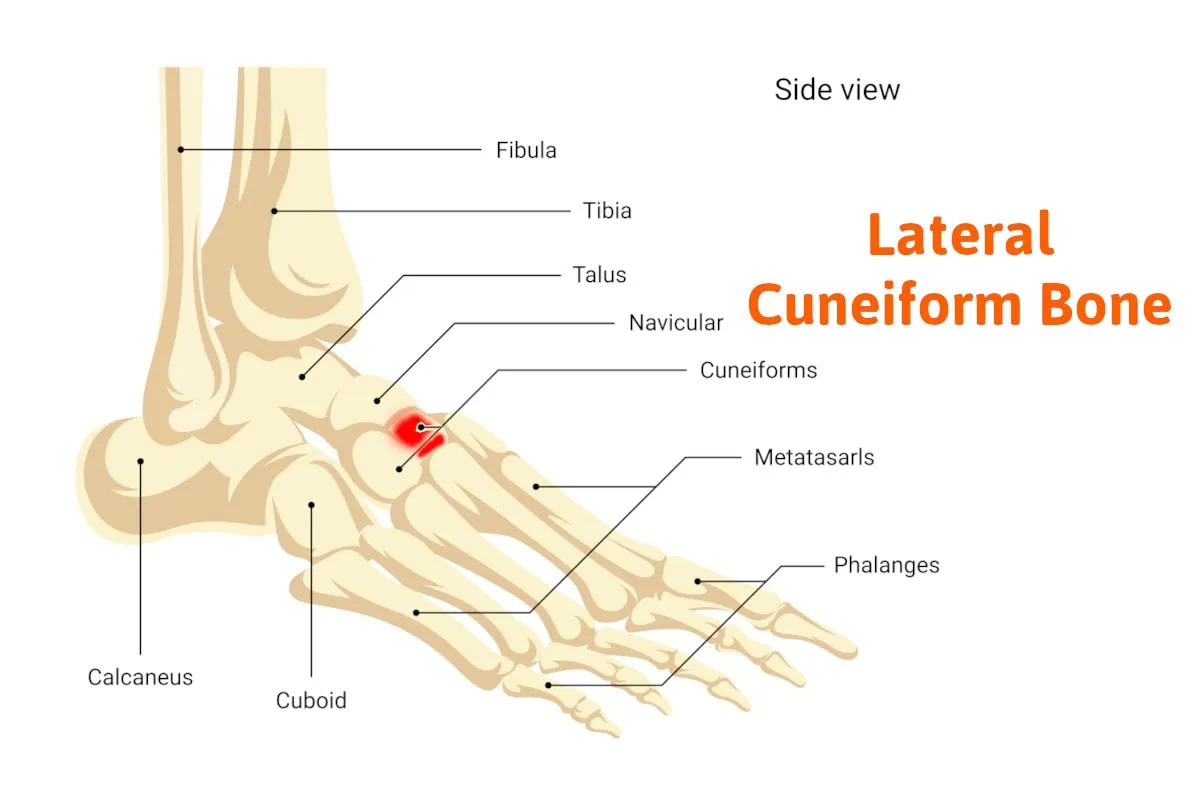
The topic of this blog is the lateral cuneiform bone. You probably have never heard of this bone. There are many bones in the human foot, 26 total. Names of foot bones that may be more familiar to you are the metatarsal bones, phalanges, calcaneus (heel bone), and talus (ankle bone). You may have heard of these bones because pain or fractures may occur in their location. The lateral cuneiform bone has a significant role in foot function, however it does its job silently. It does the work it was built to do, and you’ll seldom hear from it as it’s very rare to get injured. It’s part of a group of bones called the tarsal bones that we’ll discuss before diving into the lateral cuneiform bone specifically.
Basic foot anatomy
The foot can be separated into three separate areas. The rearfoot, is comprised of the calcaneus (heel bone), and the talus (ankle bone). The forefoot is composed of the metatarsal bones and phalanges and finally, the area in between is called the tarsal bones.
The tarsal bones. There are five bones between the rearfoot bones and the forefoot bones. Together they form the transverse arch of the foot that supports the arch. Starting towards the ankle there is the navicular bone, on the medial side of the foot, which forms a joint with the talus bone (ankle bone), and the cuboid bone which forms a joint with the calcaneus (heel bone). On the other side of the cuboid bone towards the forefoot are the fourth and fifth metatarsals that articulate with the cuboid bone forming separate joints. The cuboid and fourth and fifth metatarsals form the lateral arch. The navicular bone as we move away from the ankle towards the forefoot has three bones that articulate with the navicular to the first, second, and third metatarsals. These wedge-shaped bones are referred to as the first, second, and third cuneiforms. The medial cuneiform bone is the largest with the second being the smallest. They are also called the medial cuneiform, intermediate cuneifor,m and lateral cuneiforms.
The lateral cuneiform referred to as the external cuneiform,(middle cuneiform) which is the topic of this blog, forms the joint with the navicular bone and also the middle cuneiform medially and lies medial to the cuboid bone. It is also directly connected to the third metatarsal and does have some articulation with the second and fourth cuneiforms sharing articulation with the second and fourth metatarsals. It directly articulates with four bones. Together the four bones we just discussed form the medial arch. This arch compared to the lateral arch has more strength and can withstand more weight.
One of the functions of the lateral cuneiform bone is to serve as an insertion of the tibialis posterior tendon. The posterior tibial tendon is a very important tendon for normal foot function. It’s primary function is the support of the arch and decelerator pronation which means flattening of the foot. With part of the posterior tendons inserted into the foot on the bottom of the third cuneiform, it has an important function to stabilize the arch. Without this tendon, the foot loses much of the support in the arch. It also serves as the insertion of the flexor hallucis brevis muscle which assists in flexing the great toe downward.
Injuries to the lateral cuneiform bone
These are very rare. As I mentioned earlier it silently does its job assisting in supporting your arch. However, there is one type of injury called a Lis franc’s joint injury. Lis Franc’s joint refers to the joints formed by the metatarsal bones and tarsal bones. This injury is caused by a mechanism where the forefoot bones are forced downward in relationship to the tarsal bones. This may happen when landing on the ball of the foot forcing the ankle joint to move downward. The foot is not built well to withstand this type of force and as a result, you can suffer from multiple injuries to the bones including fractures and dislocations. This injury involves the bones and joints that form Lis Franc’s joint. In this situation, there may be an injury to the third cuneiform and its joints.
So don’t get too alarmed if you’re getting pain in your midfoot area as its most likely not from this bone. If needed the specialist may offer x-rays, MRI, or CAT scan to rule it out. However, I hope this blog gave you a better concept of the complexity of the human foot and how well if performs for us on a daily basis. You now understand the importance of the tarsal bones and more specifically the lateral cuneiform.
If you’re experiencing persistent midfoot pain or any other foot-related issues, it’s important to seek professional care. At Anderson Podiatry Center, our specialists are dedicated to diagnosing and treating foot conditions with expertise and compassion. Whether you’re in Broomfield or Fort Collins, our team is here to help you get back on your feet. Don’t hesitate to schedule an appointment today and let us take care of your foot health.
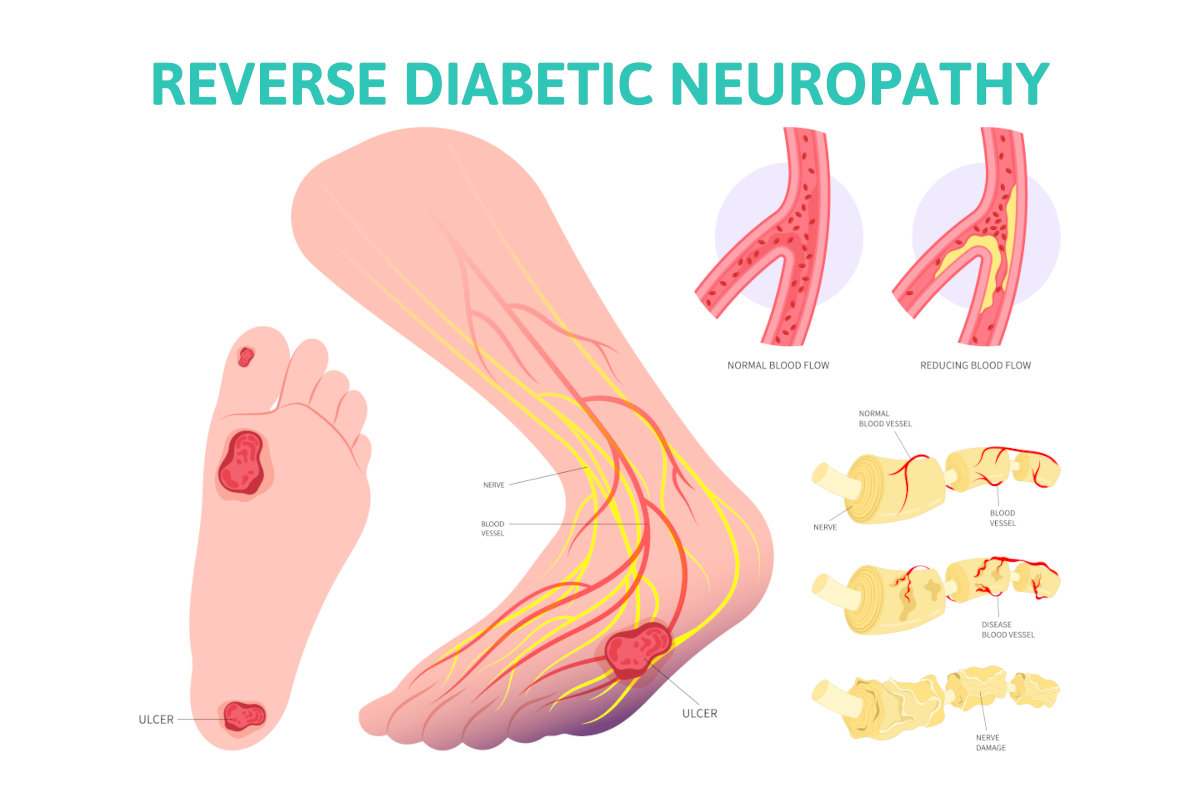
For many suffering from diabetic peripheral neuropathy, the information in this blog may be the most important you need to know when seeking treatment. We will discuss the basics of diabetic neuropathy and the conventional treatment options. However, you’ll learn how it’s reversible and we will contrast how centralized medicine continues with the same old dogma that you cannot reverse it. So, consider the other option I’ll be explaining. I will explain why I consider myself and my colleagues decentralized doctors, so you’ll better understand why centralized medicine keeps this information from you. You’ll also get access to research to prove my claim.
Approximately 50-70 percent of those suffering from diabetes will develop neuropathy. The symptoms of diabetic neuropathy will be burning, tingling numbness, and sometimes weakness in the feet and may extend above the ankles into the lower legs. The challenge is that as you lose sensation it will put you at greater risk of an amputation, the most concerning complication of diabetes.
With the nerves that control sensation your ability to feel a sore, like a callous, will be diminished. That callous may become deep, breaking down the skin and resulting in an ulcer. Then an infection may start with infection getting into bone and an amputation of a toe or portion of the foot may be necessary. Because of this risk people with diabetes are more at risk of early death from this amputation risk. The autonomic nervous system may also be damaged with diabetes. This may affect the heart, bladder, sweat glands, and sexual function.
Types of diabetic neuropathy
Small fiber disease– This is a common type of neuropathy and this term is used to describe nerve damage to the small nerve fibers that lie right beneath the skin. By taking a biopsy of the skin, the number of nerve endings can be counted to see how many are dying. Small fiber disease will cause burning tingling and numbness as the nerve endings die.
Large fiber disease – This may also occur but is not frequently talked about. This is nerve damage from compression. The compression is coming from nerve tunnels that become too tight. Carpel tunnel syndrome would be an example of this.
Type one and type two diabetes – You’ll commonly hear these terms and it’s important to know what they mean. Type 2 diabetes is most common and affects people later in life. The pancreas still makes insulin but in smaller amounts. Type 1 diabetes refers to diabetes that starts at a young age and the pancreas does not produce insulin.
Conventional treatments for diabetic neuropathy
Treatments are the following
Control diabetes – It is thought that controlling your blood sugar levels will be less damaging to the nerves and therefore the progression of neuropathy may be reduced. By controlling risk factors such as too much sugar and carbohydrate intake glucose levels can be better controlled.
Medications– medications such as Lyrica and Gabapentin are commonly recommended to control the symptoms as they become more severe. These drugs may have a positive effect on the burning tingling and numbness symptoms. In rare instances, narcotics may also be prescribed.
Medications for controlling blood sugar levels – These can vary depending on the type of diabetes you have and by controlling sugar levels less damage to the nerves may take place.
Exercise – this may improve blood flow. Also, it may help the body’s metabolism to control high blood sugars and have a positive effect on the health of the nerves. The blood vessels that supply the nerves may be better able to keep the nerves healthy. It will also reduce risk factors such as weight and high blood pressure.
Here’s what you’re being told about your diabetic neuropathy.
It’s not reversible and if you have it it’s from metabolic issues. The high glucose levels are detrimental to the nerves so the primary solution is medication to help with the symptoms. This is the centralized medical recommendation. Most of healthcare has bought into this narrative. It begins in medical schools with training of doctors to prescribe these drugs and also with the millions of dollars spent by big pharma to promote to the public. Understand the centralized concept is that big pharma along with government agencies fund the research that we fund through our taxes and then promote to you and doctors. No wonder that’s all you’re hearing.
The other new option for diabetics with neuropathy
Surgical reversal of your diabetic neuropathy. Yes, surgery can reverse your diabetic neuropathy.
The basics of nerve decompression for diabetic neuropathy.
When your blood sugars are higher than normal, glucose is broken down by another metabolic pathway called the polyol pathway. In this process, a sugar molecule called sorbitol is created. The sorbitol molecule then gets into the peripheral nerves and attracts water to the nerves. As more water is absorbed into the nerve it will swell as much as forty percent. The swelling of the nerve then creates compression on the nerve as it travels through nerve tunnels. This is why carpal tunnel syndrome is much more common in diabetics. This argument has been around for over twenty years. This information is coming from decentralized doctors like me. No drug company has funded my research, it is there to be read by all doctors and the public.
Objective research to prove that diabetic neuropathy is reversible. Me and my team of doctors have published two papers providing objective evidence of diabetic neuropathy. Two attempts were made to present this at the national meeting of the American diabetic association, and we were turned down. I was innocent enough to think we would be accepted with open arms. Obviously, there is another agenda.
The basics of our research. Patients with severe diabetic neuropathy underwent nerve decompression surgery to remove pressure on the nerves in the lower extremity. Intraoperative EMG studies were done before and then immediately after the nerve tunnel had been opened and decompressed. To do the test needle electrodes were placed in the muscle that the nerve supplied to measure how much the nerve caused the muscle to contract before and after the nerve tunnel was opened. Some patients had up to 300 percent change in this number. Again, this is objected data supplied by a machine used to measure nerve function. So, it is indisputable evidence and helps with understanding the relation to finding the right treatment for diabetic neuropathy. Here are the two studies.
Since those two studies were done there is even more research to show that patients undergoing these procedures for treatment of their diabetic neuropathy have significantly reduced the potential for an ampuation. A study by Dr. Zhang in china reports emg nerve testing before and after surgery. 1
Dr. Zhang and Dr. Anderson – Nerve Monitoring for the treatment of Diabetic Neuropathy
Amputation costs to the healthcare system can be a minimum of 80,000 dollars. Besides the monetary price, there is the cost of human life as once a limb is amputated life span is significantly reduced.
So if the centralized medical dogma could be shifted fewer drugs would be sold, fewer patients would need to go to wound care centers where many centralized medical products are used. You’re not hearing the option because if you’re a diabetic patient that is conscientious about your diabetic condition you are consulting with your doctors who manage your condition. Yet they are slow to change and have continued with the medical dogma of centralized medicine. As a peripheral nerve surgeon myself and my colleagues have patients coming to us that refuse to accept the status quo. Sadly, for new concepts to get traction and be fully accepted by the masses it takes a lot of capital.
Doctors have to be monetized so that the services we offer have a positive effect on a company or industry that collaborates with us to move the new concept forward. They win, the doctors win and so do the patients. So this relationship does not exist for doctors that do what me and my colleagues do for the treatment for diabetic neuropathy. As of yet there is no such relationship with an industry with big pockets to promote and further research what we do. Yes, for many the drugs that are used are helpful at reducing the symptoms. However they also allow for the deterioration of the nerves to continue and the risk of amputations go up! If you’d like to learn more about someone in your area who is trained as a peripheral nerve surgeon, please go the Association of Extremity Nerve surgeons website.
1 Evaluation of the clinical efficacy of multiple lower-extremity nerve decompression in diabetic peripheral neuropathy
Zhang W, Zhong W, Yang M, Shi J, Guowei L, Ma Q. Evaluation of the clinical efficacy of multiple lower-extremity nerve decompression in diabetic peripheral neuropathy. Br J Neurosurg. 2013 Dec;27(6):795-9. doi: 10.3109/02688697.2013.798854. Epub 2013 May 29. PMID: 23713665. https://pubmed.ncbi.nlm.nih.gov/23713665/
Many have heard of sciatic foot pain a term that refers to pain caused by the sciatic nerve. It’s been assumed that if you have nerve pain that radiates down your upper leg down into your lower leg and into the foot it’s likely sciatic pain. These sciatic symptoms will consist of nerve pain such as burning, tingling, and numbness that extends down to the foot causing foot pain. In many situations this may be, however, the purpose of this blog is to challenge this long-standing assumption. Yes, there may be another cause so treatment of your back with the eventual possibility of back surgery needs to be reevaluated as it may not always be the primary cause. Before we dive into this let’s make sure you have some basic understanding of sciatic foot pain.
Sciatic Foot Pain – The Conventional Approach
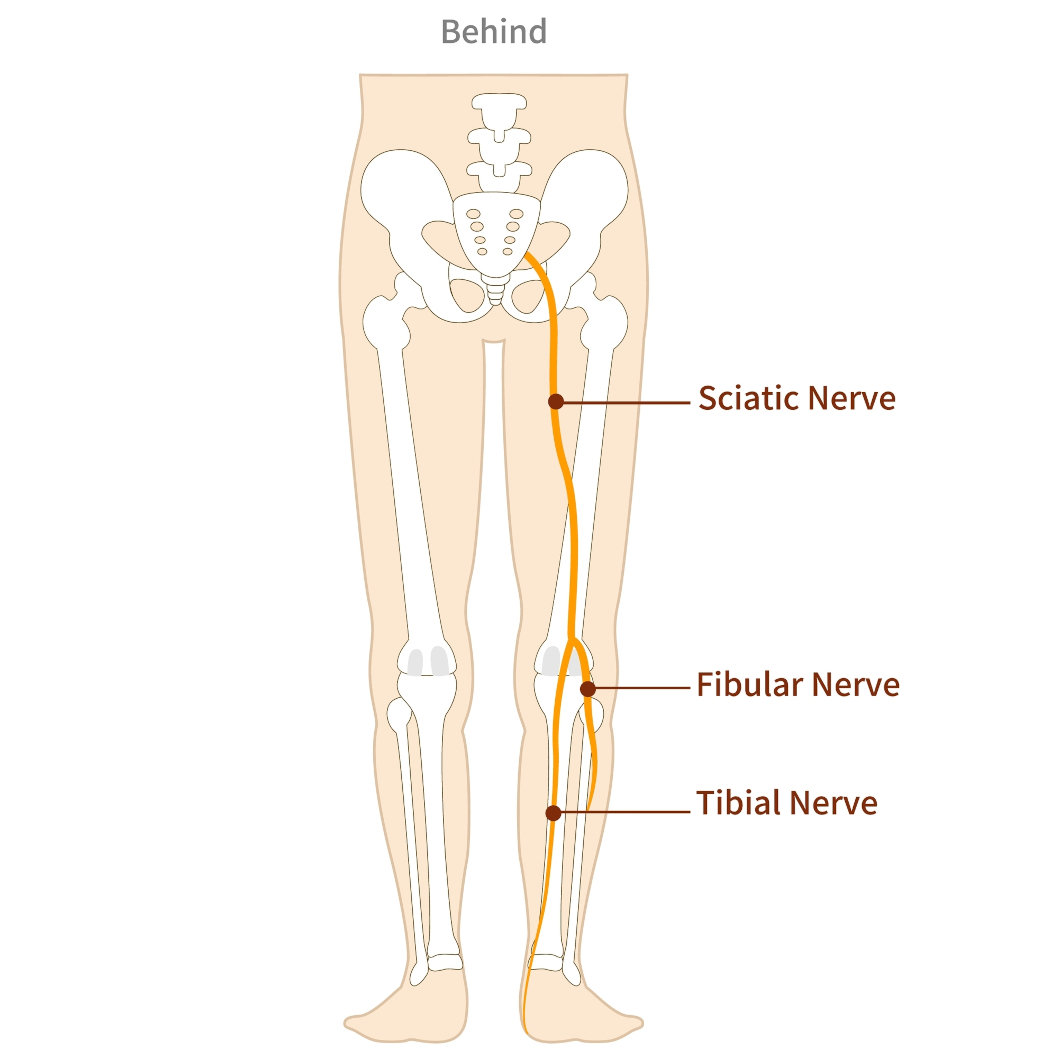
The sciatic nerve is the primary nerve that originates from the lower back. The origin is from nerve branches that originate from lumbar 1 and 2 and also sacrum 1,2,3. These branches form the sciatic nerve. There may be a herniated disk at one or more of these levels that creates sciatic pain from the nerve damage. Others may also have spinal stenosis at one of these levels or bone spurs causing pressure on the nerves.
Therefore conventionally the primary cause has always been that sciatic pain comes from pressure on the sciatic nerve as it originates from these branches. Following the nerve down into the leg it then travels down the buttock area into the back of the upper leg in the hamstring area. Just above the knee, it splits into two branches one is called the tibial nerve which travels down the back of the lower leg and eventually supplies all the nerves for the bottom of the foot. The other nerve called the common peroneal nerve travels to the outside of the knee just below the knee joint. It eventually supplies the majority of the top of the foot.
As we already mentioned this is the primary nerve that supplies nerves to the top of the foot. It’s important to note that right after it splits off from the sciatic nerve just above the knee joint and travels around the outside of the knee it goes through a nerve tunnel. This nerve tunnel is referred to as the common peroneal nerve tunnel. It’s very similar to the ulnar nerve tunnel of the elbow which patients may be more familiar with. For over two decades, I have been doing decompression surgeries on this nerve tunnel to open it and relieve pressure on the common peroneal nerve.
The common peroneal nerve can be implicated nerve conditions such as neuropathy, restless legs syndrome, and drop foot. I have been able to reverse each of these conditions by doing surgery on this nerve tunnel. Read my paper on Common Peroneal Nerve. We have also discovered that some of these patients suffering from neuropathy, restless legs, or drop foot may also be experiencing sciatica foot pain. They report nerve symptoms in the buttock area going down into the upper leg that disappear when we decompress the common peroneal nerve.
Double Crush Syndrome
A simple definition of double crush syndrome is when a peripheral nerve has one area of compression on the nerve, but another area of compression may also exist. Therefore we call it double crush . The interesting thing about this concept is that these two areas of compression affect each other. In other words, using sciatica as an example a bulging disc or bone spur may be creating compression on the peripheral nerves as they exit the spinal cord in the back and further down the leg at the location of the common peroneal nerve tunnel there is also compression sciatic pain can be reversed without back surgery. Why? By eliminating pressure on the common peroneal nerve at its tight nerve tunnel compression will still exist in the back but the sciatic nerve will be less sensitive to the compression and sciatic nerve pain will be reversed.
That is why in my many years of doing surgery on the common peroneal nerve we have noted that patients may have pain relief above the knee along the sciatic nerve into the back and also below the knee into the foot. Again there is still compression in the back that may be observed with an MRI however the nerve at the location is less sensitive and therefore the sciatic symptoms are not only relieved above the knee going into the back but also from the knee going down into the foot.
What is the significance of Double Crush and Common Peroneal Nerve Entrapment?
Avoiding back surgery – It could be that back surgery could be avoided as the common peroneal nerve is playing a larger role that was ever understood. Decompression of the common peroneal nerve would be less risky.
Failed back surgery – When back surgery has failed to eliminate sciatic pain or back pain decompression of the common peroneal nerve may be involved and offer another option rather than a repeated back surgery attempt.
How do we know if the Common Peroneal Nerve is an Issue?
Clinical examination – Patients may have slight muscle weakness, drop foot, and loss of sensation along the distribution of the common peroneal nerve. Symptoms may be present on the top of the foot and the front of the leg.
Diagnostic ultrasound – Imaging by using ultrasound may show compression at the nerve tunnel.
Emg and nerve conduction studies – These studies can sometimes show the involvement of the common peroneal nerve but are not always highly accurate.
Diagnostic injections – a new technique called the Phoenix test can be used. This involves using a small amount of local anesthesia and placing it under the skin but above the common peroneal nerve. Ultrasound guidance is used for precise placement of the anesthesia. Within minutes patients will usually respond resulting in dramatic symptom relief which will help support that the common peroneal nerve tunnel may be the root cause of the symptoms.
So if you’re trying to get relief from your sciatic foot pain that is extending into your foot it is important the consider the possibility of the common peroneal nerve being an issue. Please understand that unless you are seen by a peripheral nerve surgeon this possibly may not be a consideration.
Schedule your appointment online or call our Fort Collins and Broomfield, Colorado locations to connect with a trusted foot doctor near you at our renowned foot and ankle clinic.
Maejima R, Aoyama M, Hara M, Miyachi S. Double Crush Syndrome of the Lower Limb in L5 Radiculopathy and Peroneal Neuropathy: A Case Report. NMC Case Rep J. 2021 Dec 22;8(1):851-855. doi: 10.2176/nmccrj.cr.2021-0169. PMID: 35079559; PMCID: PMC8769459. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8769459/
A person may experience tibialis anterior pain and not consider looking into what could be causing the issue. The tibialis anterior tendon is located in the lower leg along the shin bone, tibia. It is the third largest tendon going into the foot with the Achilles tendon being the largest and posterior tibial tendon the second largest. It’s function is to pull the foot up towards the knee. Without it your foot would slap down as you walk as the heel strikes the ground. It also helps to supinate your foot as it helps to support the arch. This tendon is important for normal gait as it is needed for your foot to clear the ground as you walk or run.
Where is anterior tibialis tendonitis pain located?
For the majority of patients, the pain will be above the ankle joint along the shin bone. It may also occur in front of the ankle and down into the foot where it inserts in the foot onto the navicular bone. This bone is halfway between the great toe joint and the ankle joint. It is less common to cause pain in the foot itself.
What causes tibialis anterior pain?
Overuse – doing too much too soon can be a cause. Any activity that requires excessive use of the tibialis anterior muscle may be a cause. Because the tibialis anterior muscle is used to decelerate downward motion of the foot at the ankle joint and is used for pulling the foot upwards a the ankle joint motions that may amplify these motions may cause overuse. Example would be hiking on steep terrain as when walking downhill the muscle is used more to decerlate the downward motion of the foot so your foot doesn’t slap the ground. Racquet sports may also be more likely to cause excessive use of the muscle and tendon.
Trauma – You may also have a full or partial rupture of the tendon from and ankle injury. This could be caused by a laceration to the tendon or by any force that places excessive downward motion on the foot.
Foot types – certain foot types may be more likely to cause tibialis anterior tendonitis. Because the tendon helps to support the arch a flat foot is more likely to place excessive stress on the muscle and tendon.
Foot drop – When there is a partial or full rupture of the tibialis anterior tendon a foot drop may develop. Because the primary function of the tendon is to move the foot upwards, if it loses its function the foot will slap against the ground when walking or running. This can lead to ankle sprains as it has a significant effect on balance and stability.
How is tibialis anterior pain diagnosed?
Clinical examination– The doctor will find pain and swelling along the shin bone on the front of the leg adjacent to the tibia. Or there will be pain along the tendon in front of the ankle and down into the foot where the tendon attaches to the top of your arch. There may be pain when you pull the foot up in these same areas. If there is a partial or full tear of the tendon it may be difficult to pull the foot upwards.
Diagnostic ultrasound– This is a imaging technique that can be used to access the integrity of tendon and muscle.
MRI– The doctor may also use MRI which can very accurately evaluate a potential tear and he severity of it.
Gait analysis – simply watching you walk may help to rule out foot drop which could be caused by a tibialis anterior tear.
Treatment options for tibialis anterior pain
Rest and anti-inflammatories – this can be useful if the pain is not long term and the pain is mild.
Immobilization – Using a Cam walker to walk in can also be helpful as it will help rest the tendon and muscle.
Modification of activities – Choosing another activity or decreasing the activity that may have contributed to the problem may be recommended.
Orthotic devices – Custom made arch supports may help to reduce the stress placed on the tendon as it may be overused in attempting to support the arch of the foot.
Physical therapy – different physical therapy modalities may also be helpful.
Laser treatment – Use of MLS laser for pain treatment has also been proven successful in our practice for tendonitis issues.
Surgery – When a tear or partial tear is present surgery may be recommended to maintain the integrity of the tendon. This type of surgery may require non- weight bearing for minimum of 4 weeks.
Tendonitis versus tendinosis – We now know that what was once thought to be an inflammatory issue , tendonitis may be incorrect and in fact it’s more likely that the tendon is breaking down. There may be small microscopic tears in the tendon. This is often referred to as tibialis anterior tendonopathy. For close to two decades now we have had great success with the use of Human Cellular tissue products.
What are human cellular tissue products?
Sometimes referred as stem cell treatment this can alleviate the need for surgery. When there is severe pain along the tendon, and the MRI or ultrasound reveals tears this treatment can be used. This form of treatment has greatly reduced the need for the surgical repair of tendons in our practice. It is not suggested for a full tendon tear but when the tears are minor or partial it can work extremely well.
How would human cellular tissue products be used?
This is done in a clinic setting. The area where the tendon tear is located is numbed with local anesthesia so it’s a pain free experience. Then with the use of diagnostic ultrasound to locate the area of tendon damage the stem cell product is injected into the area. The patient is allowed to walk immediately and uses a Cam walker to walk in for four weeks.
So consider these options if you have tibialis anterior pain. And one last consideration is to avoid the use of cortisone in the area of the tendon. I do not consider this a good option as it can potentially weaken the tendon and perhaps cause a rupture.
Easily schedule your appointment online or contact our skilled foot doctors at the nearest foot and ankle clinic in Fort Collins or Broomfield, Colorado to find the best podiatrist near you.
Toenail fungus is one of the most common complaints that are seen by a podiatrist. The yellow discoloration can be embarrassing to many. The nail can also become very thickened and even painful because of the thickness. It can also lead to a greater chance of a nail becoming ingrown because of how the nail becomes deformed. So how do you decide on toenail fungus removal?
Causes – fungus likes a warm dark and moist place to live. And for many this is the environment our feet are in daily. Many will feel like they get the infection from a dirty locker rooms or a nail salon. Yes, this is a possibility for the fungus to infect nails but the more we understand this problem, the more we believe it is about your immune system. Some immune systems may not be as capable of fighting a fungal infection. Antidotal evidence for this is supported by the fact that with married couples one person may get the fungal nail infection while the other bed mate never does. It’s also a common story to hear that, “my father had this when he was my age so now, I must be getting it also.” Ideally if we know of better ways to positively improve our body’s immune system improve it we may have better solutions. So, for now, there are four primary treatments I will discuss. And tell you things you may consider doing to lower your risk.
How to I know if I have toenail fungal infection?
The nails will become discolored. It’s most common to see a yellow discoloration on the nail but it may also have a white or darker appearance. Psoriasis can mimic a fungal nail appearance. This is an autoimmune disease usually accompanied by plaque formation on both legs and arms.
How is fungal nails diagnosed- For most patients the appearance of the toenails will be used to determine is fungus is the issue. Some doctors will do nail cultures, but this may not always be highly accurate.
Things to do to prevent toenail fungus
Avoid being in shoes all day. Because this can be a dark moist place it may create a better environment for fungus to start.
Clean your feet- It may sound too simple but when you shower, or bathe be sure to use lots of soap and water on your feet. Be sure to adequately dry them before you return to shoes and socks.
Avoid nail polish as this can be unhealthy to the nail and make you more prone to fungal infections. There are however some nail polishes that have antifungal agents in it that may be a good replacement.
Try over the counter topicals – If it’s early stage and not too severe products such as Lamisil may be useful. Tea tree oil is also considered as another over the counter topical option. You may also want to consider antifungal shoe spray to use in your shoes. This may help reduce any fungus you may have in your shoes.
Options that your foot specialist may offer for toenail fungal removal
Topicals- when treating toenail fungus when it’s not severe these may be effective. The challenge with any topical is its ability to get absorbed into the nail. So, whatever is in the topical may have limited effect because of the absorption challenge. We currently use a product called tolcyleyn produced by marlinz pharma that can only be purchased exclusively through podiatry clinics. It has a patented compound that allows for better absorption, it is very common for doctors to prescribe antifungal topicals such as jublia. This may have limited effects especially in more severe cases.
Oral antifungal medications- These are more effective than topicals but have added side effects including liver toxicity. Before this option is considered for toenail fungus removal, most doctors will order blood tests (liver panel studies) to ensure there is no current damage to the liver and follow-up with this study during treatment. The most common medication for oral use is called terbinafine Lamisil.
Surgery- in special situations the doctor may suggest permanent removal of the affected nail. Especially in the senior population, this may be a good choice if it’s only one or two nails and the patient is not concerned about the cosmetics. Often the nail may be so damaged and thickened that that appearance is improved. This is an office procedure, and the patient can return to normal activities almost immediately. A chemical is applied to the nail bed where the nail was removed to kill the cells that make the nail preventing it from regrowing. There are no sutures or pain pills required and for most the toe is fully healed in 2-3 weeks. For many, the option to remove the nail may be a good option.
Consumer beware. Before we discuss the third treatment option I’d like to share and observe in the medical world today. Many of you frequently offer your concerns about big pharma whether it’s with concerns the Covid vaccine or treatments for covid not to mention concerns with continued marketing efforts for drugs in other arenas. It may be no different in the treatment of toenail fungus. Doctors are monetized to offer you prescriptions for oral medication or prescriptions of topicals. Again, topicals have a low success rate and although oral medication is better, you’re challenged with potential liver damage. The message for you is understand is that before we discuss what I consider the best option. You may not have heard much about it as big pharms cannot monetize doctors when it is performed. There may be a lot of influence to keep you from not considering what I consider the best option. Laser treatment.
Laser treatment – for over 16 years we have been offering laser as an option for toenail fungus removal and believe it has the highest cure rate. We use the Pinpointe laser which destroys the fungus because of the heat it generates. It pulses light into the nail very rapidly. Much like touching a stove very quickly, you don’t feel the heat during treatment. Because toenails take at least 9 months to fully grow out it takes that long to see how effective a treatment is. From our experience we have discovered everyone needs at least three treatments. Therefore, we do the first two treatments one month apart and that is followed by a third treatment three months after the second. For minor cases three treatments may be all that is needed but more severe cases may need more. Don’t get stuck searching for ‘laser toenail fungus removal near me‘ and not finding a certified and experienced podiatric practice. Our patient testimonials on youtube are from patients just like you!
Yes, toenail fungus can be frustrating however if you get started on treatment sooner than later, you’ll increase your chances of success. Also consider laser as the best option understanding that information out there to promote medications or products to apply to your nail may be drowning out laser as the most successful option you may have. Schedule your appointment online or call our Fort Collins and Broomfield, Colorado locations to connect with a trusted foot doctor near you at our renowned foot and ankle clinic. Consider our years of experience when dealing with toenail fungus removal!
Heel pain is one of the most common foot complaints. Plantar fasciitis, which is a thick band of tissue that connects to the heel on the bottom of your foot, is more frequent to experience pain rather than on the back of the heel. We will discuss what are the various conditions that cause pain on the back of the heel and what treatment options are available. For many of you what we discuss will differ from a lot of the conventional ideas and treatments you may have heard about. If you’ve heard that surgery may be needed for this condition, and you want to avoid it, this blog is for you. To understand our approach, we need to start with what is the cause.
The root cause of pain in the back of the heel.
There are three primary types of heel pain. The diagnoses that we will discuss, Haglund’s deformity, retro calcaneal spurs and Achilles tendonitis.
When you walk your foot pronates and supinates. With pronation that occurs from heel strike to the point where the ball of your foot has your body weight transferred onto it, the heel bone rolls inward. Then when you start to propel forward and roll up on the ball of the foot the heel bone is rolling outward. This twisting torsion is thought to cause friction between the Achilles tendon and the back of the heel bone. If you look at the back of your heel the lower half of the heel is where the Achilles tendon is attached, and the upper half is where it can rub against the bone. This rubbing is thought to be the source of the three primary diagnosis. This rubbing can create a breakdown, damage, to the Achilles tendon either where it begins to attach to the bone or just above this area where the bone rubs against it. Microtears are thought be created within the tendon when this occurs. Or in the situation with Haglund’s deformity or a retrocalcaneal spur extra bone will be created that is seen on x-ray.
Haglund’s deformity- this term is used to refer to an enlargement on the back of the heel in the area where the Achilles attaches to the back of the heel bone. This bump tends to be towards the outside of the back of the heel adjacent to the Achilles tendon, however it can be located throughout the back of the heel bone making it appear to be larger than normal. This can be seen on x-ray.
Retro-calcaneal spur- This is a condition where there is a spur on the back of the heel bone where the Achilles tendon attaches to the heel. This can be seen on an x-ray. Clinically the size of the spur may not present as large as Haglund’s deformity on the back of the heel. The pain is right beneath the Achilles tendon on the back of the heel. Whereas Haglund’s deformity tends to not only cause pain directly over the Achilles area but also on one or both sides of the heel bone adjacent to the Achilles.
Achilles tendonitis– Of the tendons and muscles in the foot and ankle the Achilles tendon is very important. It’s the largest tendon in your body and important for normal ambulation. It connects the calf muscle to the foot. The two calf muscles attach to the Achilles tendon. This occurs when there is pain and swelling on the Achilles tendon on the back of the heel bone. X-rays will not show any boney abnormality which eliminates the diagnosis of Haglund’s deformity or a retrocalcaneal spur.
Achilles bursitis- This is a condition that causes pain between the heel bone and the Achilles tendon. For some this condition is created by the Achilles tendon rubbing against the heel bone. The fluid filled sac called a bursa evolves as a reaction to this. Much like a blister on your skin when the skin is rubbed a lot. Treatment for this can be resting anti-inflammatories aor a cortisone injection.
Severs’ disease– this happens before the foot is fully grown. Children will frequently complain of pain in the back of the heel. It will usually occur with activity and go away when inactive. It’s a frequent complaint when they start sports such as soccer, basketball, and volleyball. Another name for this is calcaneal apophysitis. The pain that occurs is from inflammation to the growth plate in the heel bone(calcaneus). Treatments may include anti-inflammatories, resting and immobilization. However, orthotics are the most successful option for many. These custom-made inserts support the foot and Achilles tendon area so that the connective tissue structures that attach to the heel bone are no longer causing tension on the growth plate.
Diagnosis of these conditions
X-ray- this can help to determine if there is any extra bone present in the case of Haglund’s deformity or a retro calcaneal spur.
Diagnostic ultrasound. This is useful to evaluate if there is damage to the Achilles tendon.
MRI- This can give more detail than an ultrasound to evaluate the quality of the Achilles tendon.
Clinical examination- There can be pain and swelling on the back of the heel. Shoe gear will tend to rub against this area and cause pain.
Treatment for Haglund’s deformity, retrocalcaneal spur and Achilles tendonitis.
Conventional treatments have included the following-
Resting
Icing
Physical therapy
Immobilization
Non steroidal anti-inflammatory
Orthotics
Be sure you have properly fitting shoes and supportive shoes . Avoid activities that require tight fitting shoes such as ski boots or ice skates. Trying over the counter shoe inserts may also help.
All of these can have a positive impact but may not be dealing with the root cause of the problem.
The root cause. As was mentioned earlier we now believe that the cause of pain on the back of the heel for most can be from the rubbing of the Achilles tendon against the heel bone. Yes, you may see an enlargement on the back of the heel and for some there may also be evidence of an extra amount of bone or a spur however our non surgical treatment success disputes that the bone is the problem. There are three options that we feel have the greatest chance to eliminate pain on the back of your heel and eliminate the need for surgery. MRI has proven the problem is with the tendon not the bone.
MRI- MRI has demystified why we have so much success with our treatments and can almost eliminate surgery. MRI has constantly shown us that there is no inflammation to the tendon which would indicate tendonitis but rather the findings are more consistent with micro tearing of the tendon. This indicates breakdown of the tendon on a microscopic level.
Here are the big three treatments to prevent surgery for pain in the back of the heel
Orthotics- by very precising controlling the torsion(rolling) of your heel bone against the Achilles we are truly reducing the irritation to the Achilles tendon. structurally speaking the orthotics correct and reduce the structural issue that led to the pain. By reducing the rubbing of the heel against the tendon many get reversal of pain with this treatment.
Regenerative medicine- This is commonly referred to as human cellular tissue product treatment. We commonly inject into the damaged tendon, umbilical cord or placental cell tissues that help to repair the damaged tendon. This may be done in combination with orthotics. The orthotics help to eliminate what caused the problem and regenerative medicine repairs the damage. See our patient testimonials for heel pain relief after regenerative medicine on youtube.
Shockwave treatment- This technology uses powerful soundwaves to create mild trauma to the tendon and by doing so this stimulates the body’s reparative mechanisms to repair the tendon. This usually involves three separate treatments at weekly intervals.
If your pain is getting worse and you’re having it for long periods of time. You may be tired of trying different shoes to get rid of your heel pain have been told surgery may be in your future, please consider these other options. We have shown many of our patients that surgery is not necessary for the vast majority. With two clinical foot locations in Broomfield and Fort Collins, you won’t need to wait because we are accepting new patients/existing patients for same or next day appointments to see you local foot doctor. Rest assured when looking for a “foot doctor in fort collins”, our patients will agree that we are caring, experienced and knowledgeable in the latest innovations of foot care.
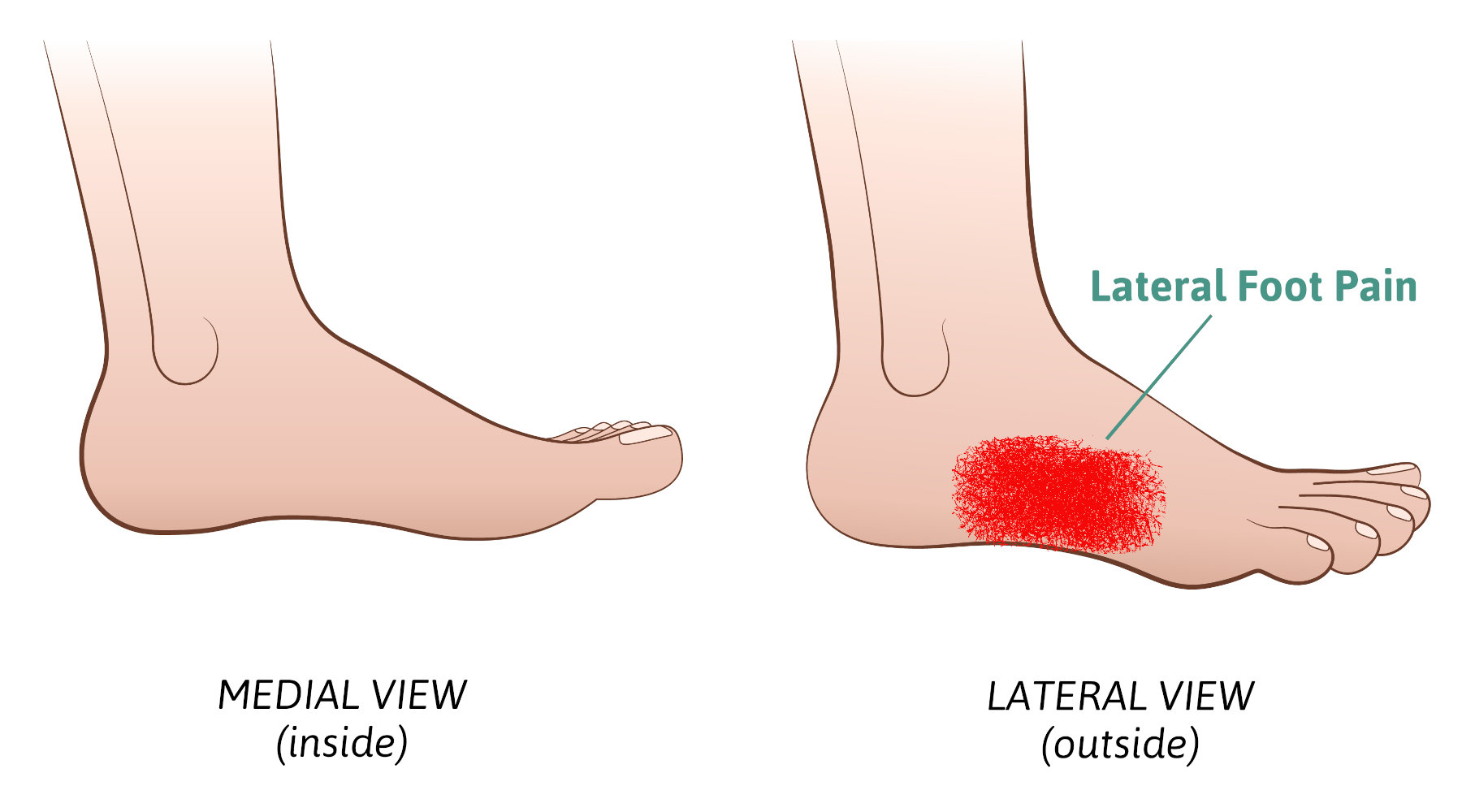
Lateral foot pain refers to the pain being on the outer side of the foot. This means anywhere from the small toe joint back to the heel bone area. Any pain that is along the outer edges of the foot. This blog will review many problems that can arise in this region of the foot. However, before we get started it’s important to point out that lateral foot pain in many cases may be related to a problem elsewhere in the foot. This other issue is creating a situation where you have difficulty walking and favor the painful area by rolling your foot towards the outside. This may create stiffness and pain in the lateral foot. So as a foot specialist I’m always looking to find in the patient’s story, their history, was there some other type of pain that preceded the lateral foot pain. Here are six things that cause lateral foot pain and treatment options.
Cuboid syndrome – This pain is usually associated with the calcaneal cuboid joint. This joint lies on the outside of the foot at the highest part of your arch on the lateral side of your foot. The history of plantar fasciitis is commonly associated with cuboid pain. By favoring the foot and walking on the outside of the foot the reducing the pulling of the plantar fascia from the bottom of the foot and thus significant stress is placed in this area. AS the heel pain is reduced the cuboid pain increased. Treatment therefore should start by addressing and eliminating the heel pain and the cuboid pain will fix itself.
Peroneal tendonitis – The peroneal tendons lie on the outside of the foot coming from behind the fibula bone and then coursing on the outside of the heel One these tendons, the peroneus brevis’s attaches to the base of the fifth metatarsal, the large eminence that protrudes halfway between the ball of your foot and the heel. The other tendon, peroneus longus runs beneath the arch and attaches to the base of the first metatarsal bone and helps to pull this bone downward to support the medial arch. Basically, both tendons are like stirrups helping to stabilize the foot from moving side to side. Any activity that requires along side-to-side motion can stress these tendons and, in some situations, they can develop tears. Flat feet may also contribute to peroneal tendonitis. We have found that human cellular tissue products are a great option to help repair these tendons so surgery can be avoided.
Fractures – Fractures of the heel bone cuboid bone or fifth metatarsal can all cause pain in this area. Of these three fifth metatarsal bone fractures are the most common.
Fifth metatarsal bone fractures – these are usually associated with an ankle sprain where the twist is so forceful the peroneal brevis bone that attaches to the base of the fifth metatarsal pulls a portion of the fifth metatarsal away from the rest of the bone. This is referred to as an avulsion fracture. The other type of fracture referred to as a Jones fracture occurs when upward force is placed primarily on the fifth metatarsal and not the other metatarsals causing the bone to fracture just behind the base of the bone. An example would be a basketball player landing on another player’s foot with all the body weight on the fifth metatarsal. Both these fractures require immobilization in a cast or Cam-boot and the probability of surgery to repair the fracture is more common with the Jones fracture.
Cuboid fractures – This bone is between the heel bone and the fifth metatarsal. Fractures here are very uncommon and may be associated with trauma but more likely may be caused from overuse.
Treatment for lateral foot pain is usually immobilization
Calcaneal fractures – The calcaneus is your heel bone and fractures can occur from trauma such as a fall and when severe may require surgery. However, in most cases overuse can cause stress fractures the heel. The heel bone is very vascular, so the bone tends to heal very well.
Sinus tarsi syndrome – This is very common and is associated with the subtalor joint. This joint lies beneath the ankle joint and is the joint that allows your foot to move like a universal joint on a care. In all different body planes. There are two ligaments in the joint that are thought to become inflamed from overuse or trauma such as an ankle sprain. It’s not uncommon for someone to report an ankle strain weeks or months ago but the pain may linger in this location. Treatment with cortisone injections and custom-made arch supports called orthotics successfully eliminates the pain.
Sural nerve pain – This is a nerve that originates in the lower leg and travels down the side of the foot to the small toe. This nerve can be irritated. By a multitude of different types of traumas including, Surgery with an incision being placed on the outside of the foot or ankle. From an ankle strain causing the nerve to be stretched. Surgery or trauma such as being kicked in the lower leg. Treatment may include, cortisone injections, laser treatments and when pain is severe and conservative measures fail, surgery removal on the nerve in the leg and burying into muscle to prevent regrowth.
Great toe joint pain – This requires its own special category as any pain in the great toe joint area will cause you to walk differently. Because normal ambulation requires a significant amount of body weight to be transferred onto the great toe joint, anything that alters the normal gait pattern can cause significant lateral foot pain. This would include the following
Bunion pain – this occurs when the great toe angulates towards the second toe and a bump is created at the base of the great toe joint. Shoes will cause irritation to the bump.
Sesamoiditis – There are two sesamoid bones the sit beneath the great toe joint and function like the kneecap to improve the strength of the muscles that pull your great toe down. This can become painful for many reasons. Again, you’ll tend to reduce the load on these bones and transfer your weight laterally.
Hallux rigidus – Hallux refers to the great toe and rigidus refers to great toe joint having limited motion. When the great toe cannot move up adequately for normal gait you’ll have to transfer weight to the outside of your foot. Treatment for all three of these conditions may include custom made arch supports, orthotics, to reduce pain and improve function. Cortisone injections. Human cellular tissue products to reduce joint pain for Hallux rigidus, see our video below. Or surgery is another way to correct the problem.
Treatments for lateral foot pain
In the early stages taking anti-inflammatories and physical therapy may help reduce swelling along with an elastic bandage early on.
Reduction of physical activity may also be useful.
Use of shoe inserts may be useful in a treatment plan..
Final thoughts. So, if you’ve been dealing with lateral foot pain and are not sure what it is and what treatment choices you must consider consulting with a foot and ankle specialist. Finally remember you could be wasting a lot of time and money treating lateral foot pain that is failing because it never was the primary problem. Give us a call at one of our local foot and ankle clinics in Fort Collins and Broomfield. We see patients searching for ‘the best foot doctor’ from all across the tri-state area, such as Wyoming, Cheyenne and Loveland. With over 10600+ views on Youtube and a large Facebook community, we are always looking to provide real solutions for all our patients foot ailments.